Practice Labeling the Ear
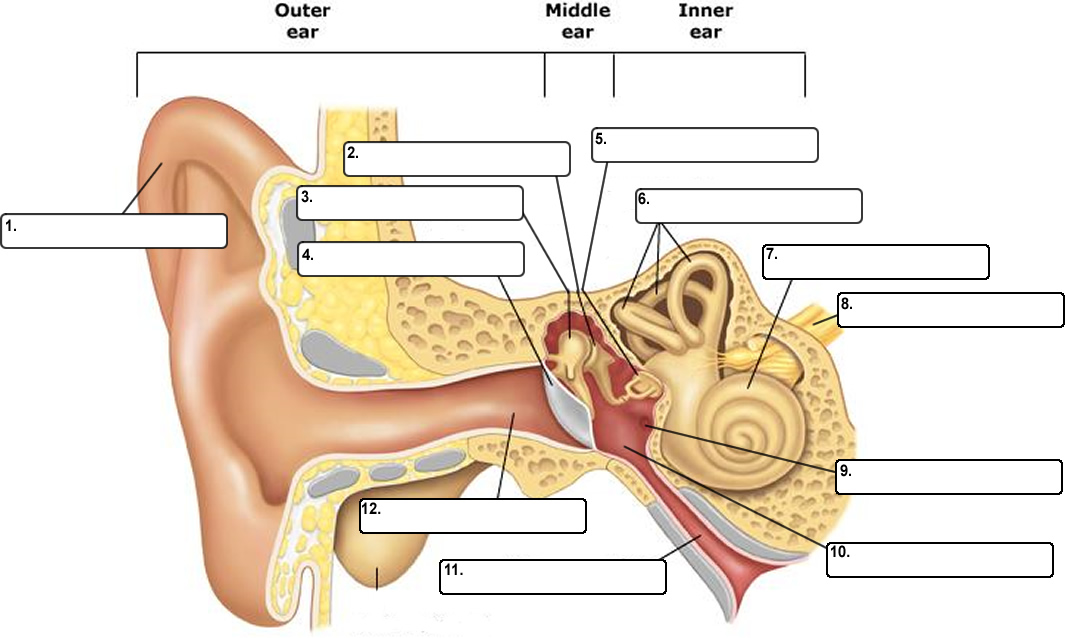

Tympanic Membrane
Auricle
Auditory Canal
Eustachian Tube
Round Window
Tympanic Cavity
Cochlea
Semicircular Canals
Vestibulocochlear Nerve
Malleus
Incus
Stapes
![]()
Other Resources
Ear Anatomy - Drag and Drop Labeling